

Translate this page into:
Seborrheic Keratosis with Bowenoid Transformation
*Corresponding author: Siddharth Mani, Department of Dermatology, Indian Naval Hospital Ship Sanjivani Kochi, Kerela, India. smani5931@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Mani S, Rout A, Khandare M, Mahto H. Seborrheic Keratosis with Bowenoid Transformation. Indian J Postgrad Dermatol. doi: 10.25259/IJPGD_73_2024
Abstract
A 30-year-old male presented with multiple, raised, hyperpigmented lesions on the penis and scrotum for 6 months. Physical and dermoscopic examinations revealed verrucous papules with distinct patterns. The histopathology report was consistent with the diagnosis of seborrheic keratosis (SK) with bowenoid transformation. Human papillomavirus (HPV) typing revealed HPV 6. Initial treatment with imiquimod 5% did not have any response. Later radiofrequency ablation led to complete resolution of lesion. SK, a benign epidermal tumour, is linked to factors such as sun exposure, HPV and genetic mutations. Studies suggest a potential for malignant transformation in SK, especially with HPV 6, as seen in this case, underscoring the need for patient follow-up and counselling.
Keywords
Bowenoid transformation
Human papillomavirus
Seborrheic keratosis

INTRODUCTION
Seborrheic keratosis (SK) is a benign epidermal tumour whose exact aetiology is unclear; however, many incriminating factors have been proposed which include but are not limited to sun exposure, human papillomavirus (HPV) and genetic mutation.[1] fibroblast growth factor receptor 3 and phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha (FGFR3 and PIK3CA) activation are the most common genetic mutations associated with SK.[2] These genes are also implicated in many carcinomas as melanoma, bladder carcinoma, lung carcinoma and colon cancer, just to name a few. HPV 6 has been commonly detected in SKs occurring on genital skin; nonetheless, the association is not strong for its non-genital counterpart.[3]
CASE REPORT
A 30-year-old male presented with multiple, raised, hyperpigmented lesions over the penis and scrotum of 6 months duration [Figure 1]. The lesions were asymptomatic and gradually increased in size and number. Physical examination revealed multiple, poly-sized, discreet, hyperpigmented and verrucous papules present over the scrotum and penis. Dermoscopic examination revealed the presence of a finger-like exophytic papillary pattern, moth-eaten borders, scales and comedo-like opening in a larger lesion [Figure 2a]. The smaller lesion had a cerebriform pattern with few comedo-like openings [Figure 2b]. A biopsy was performed with the differentials of SK, bowenoid papulosis and condyloma accuminata. Histopathological examination at low power (×10) [Figure 3a] revealed acanthosis, hyperkeratosis and a horn cyst in the epidermis suggesting SK. However, a few atypical cells were present suggesting bowenoid transformation.
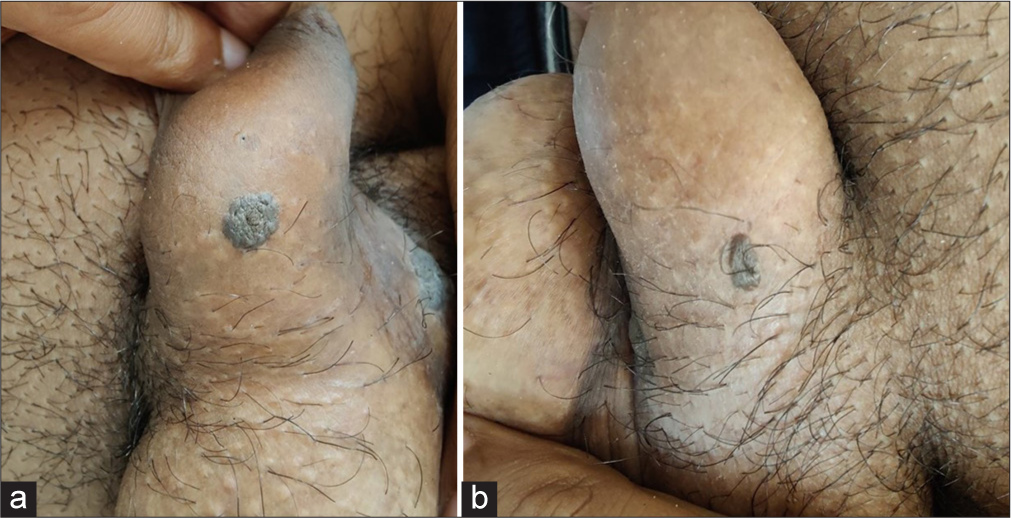
- (a and b) Multiple, poly-sized, discrete, hyperpigmented, verrucous papules present over scrotum and penis.
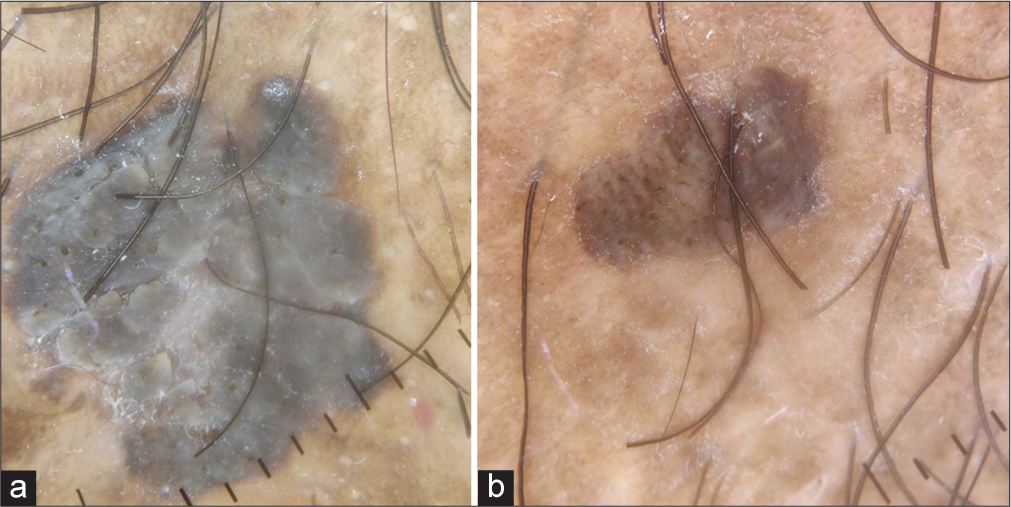
- Dermoscopic examination of larger lesion revealed (a) presence of finger like exophytic papillary pattern, moth eaten borders, scales and comedo-like opening while the smaller lesion had (b) cerebriform pattern and few comedo-like openings on dermoscopic examination.
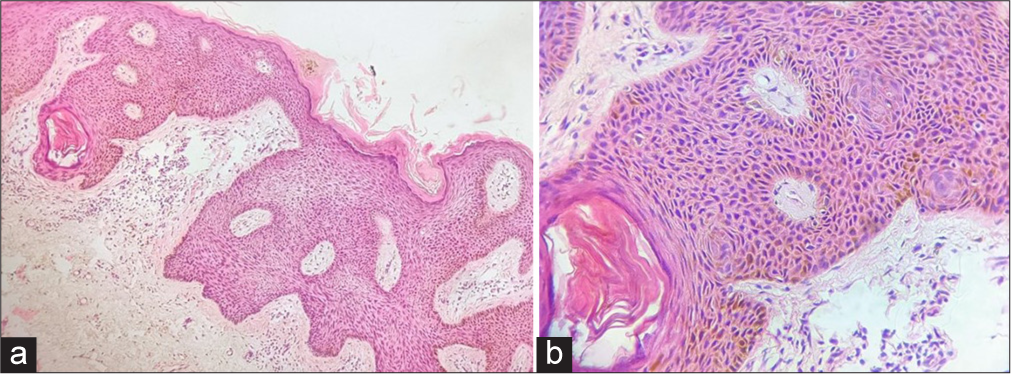
- Histopathological examination at low power (×10) (a) revealed acanthosis, hyperkeratosis and a horn cyst in epidermis suggesting seborrheic keratosis with a few atypical cells scattered along the epidermis suggesting Bowenoid transformation while, at high-power (×40), (b) epidermis appeared to be in disarray with atypical cells scattered throughout the thickness of epidermis and poorly formed keratin pearls.
At high power (×40) [Figure 3b], epidermis appeared to be in disarray with atypical cells scattered throughout the thickness of the epidermis and poorly formed keratin pearls. HPV typing revealed the presence of HPV 6. The patient was diagnosed as a case of SK with bowenoid transformation. He was given cream imiquimod 5% thrice a week for 12 weeks, but he failed to show any response. Later, a radiofrequency ablation was done which resulted in complete resolution of the lesion and the patient has not shown any recurrence in the past 6 months.
DISCUSSION
Multiple studies have elucidated the possibility of malignant transformation in SK. Malignant melanoma, squamous cell carcinoma, basal cell carcinoma, keratoacanthoma, Bowen’s disease and eccrine carcinoma have been reported to be associated with SK.[4] In a study by Vun et al., 813 histological cases of SK were studied out of which 43 were associated with non-melanoma skin cancer.[5]
Wu et al. reported a total of 17 cases (0.9%) of bowenoid transformation out of 1904 SK cases. Most cases (11) were on sun-exposed parts and five patients were HPV positive.[6] The study also mentioned strong expression of p16, p21, p53, ki-67 and cyclin D1 in SKs with bowenoid transformation. To distinguish between micro clonal variant of SK micro clonal variant of seborrheic keratosis (MSK) and pagetoid Bowen’s disease (PBD), ki67 and p16 markers can be used. High expression of p16 and Ki-67 or p16 alone favours the diagnosis of PBD over MSK. Our patient could not afford IHC with regard to ki-67 due to poor financial status. In a similar study by Rajabi et al., 429 SK cases were retrospectively studied and six cases showed malignant change. Out of these six cases, five had the histopathological features of bowenoid change.[7] In our case, histopathological features of bowenoid transformation overlapping with SK were present. Genital SK is more commonly associated with HPV 6 as compared to its non-genital counterpart. In the study conducted by Tardío et al., 28 out of 40 genital SKs had HPV 6 while only two out of 20 extragenital SKs demonstrated the presence of HPV.[3] We also detected HPV 6 in our case. HPV is associated with epithelial precancerous lesions. Type 6 of HPV is low risk with its role being limited to causation of genital warts. However, in a systematic review published by Da Silva et al., HPV 6/11 individual or dual infection is associated with penile and laryngeal carcinomas. E5, E6 and E7 proteins of HPV have a major role in the pathogenesis of carcinoma. In the genomic study of HPV 6/11/16, it was found that there was no similarity between E5 and E6 of low-risk HPV 6/11 and high-risk HPV 16. However, the E7 oncogene appeared to be more conserved between these three and the similarities observed in the E7 oncogene could help explain why HPV6 and HPV11 seemed to show some carcinogenic potential.[8]
In our case, even though the clinical and dermoscopic features pointed to SK, biopsy results showed the presence of bowenoid transformation.
CONCLUSION
The case highlights the importance of the possible association of genital SKs with HPV and possible malignant transformation. These cases need to be under follow-up for some time and patients need to be counselled regarding early visits to the hospital on the recurrence of old lesions or appearance of new lesions.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- The Prevalence of Seborrhoeic Keratoses in an Australian Population: Does Exposure to Sunlight Play A Part in their Frequency? Br J Dermatol. 1997;137:411-4.
- [CrossRef] [Google Scholar]
- Oncogenic PIK3CA Mutations Occur in Epidermal Nevi and Seborrheic Keratoses with A Characteristic Mutation Pattern. Proc Natl Acad Sci. 2007;104:13450-4.
- [CrossRef] [PubMed] [Google Scholar]
- Genital Seborrheic Keratoses are Human Papillomavirus-related Lesions. A Linear Array Genotyping Test Study. APMIS. 2012;120:477-83.
- [CrossRef] [PubMed] [Google Scholar]
- Malignant Neoplasms Associated with Seborrheic Keratoses. An Analysis of 54 Cases. Am J Dermatopathol. 1996;18:278-82.
- [CrossRef] [PubMed] [Google Scholar]
- Seborrhoeic Keratosis and Malignancy: Collision Tumour or Malignant Transformation? Australas J Dermatol. 2006;47:106-8.
- [CrossRef] [PubMed] [Google Scholar]
- Seborrheic Keratosis with Bowenoid Transformation: The Immunohistochemical Features and Its Association with Human Papillomavirus Infection. Am J Dermatopathol. 2015;37:462-8.
- [CrossRef] [PubMed] [Google Scholar]
- Bowenoid Transformation in Seborrheic Keratosis: A Retrospective Analysis of 429 Patients. J Res Med Sci. 2012;17:217-21.
- [Google Scholar]
- Malignancy Associated with Low-risk HPV6 and HPV11: A Systematic Review and Implications for Cancer Prevention. Cancers (Basel). 2023;15:4068-70.
- [CrossRef] [PubMed] [Google Scholar]




