

Translate this page into:
Excising Persistent Discoid Lupus Erythematosus Lesions: Nipping Evil in the Bud
*Corresponding author: Tanya Jain, Department of Dermatology, Government Medical College and Hospital, Chandigarh, India. jain.tanya310@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Jain T, Arora A, Aneja S, Thami GP. Excising Persistent Discoid Lupus Erythematosus Lesions: Nipping Evil in the Bud. Indian J Postgrad Dermatol. 2025;3:90-1. doi: 10.25259/IJPGD_71_2024
Dear Editor,
Discoid lupus erythematosus (DLE) presents as erythematous scaly patches that heal with atrophy, pigmentary changes and scarring predominantly over photo-exposed sites.[1] DLE lesions are at risk of developing squamous cell carcinoma (SCC) with an incidence of 2.3–3.3% which is four-fold as compared to the general population and interval of developing SCC from DLE is 4–20 years.[1,2] The most common site of this malignant transformation is scalp followed by lips.[3] Hypertrophic or verrucous DLE lesions are more associated with malignant transformation, hence making total excision a more reliable treatment option. In past, longstanding verruciform lesions of DLE with no obvious progression responded favourably to surgical excision with minimal recurrence.[4] A similar approach was followed for persistent, treatment refractory lesion in our patient.
A 65-years-old female, a known case of DLE on treatment since 6 years with potent topical corticosteroids and hydroxychloroquine complained of a persistent single erythematous, scaly nodulo-plaque lesion surrounded by hypopigmentation and hyperpigmented border on the centre of lower lip [Figure 1a]. Biopsy from the lesion in March 2022 was reported as consistent with DLE. She was treated with hydroxychloroquine and methotrexate along with three injections of intralesional steroid but no improvement was observed till August 2022. It was then decided to excise the lesion as a therapeutic measure and allow healing by secondary intention. The wound healed well with secondary intention in 1 month [Figure 1b]. The histopathology of the excised lesion showed malignant changes developing moderately differentiated SCC showing a hyperkeratotic epidermis which, at places, was hyperplastic and dysplastic along with invasive tumour with keratin pearls [Figure 2]. The patient was referred to radiation oncology for further management.
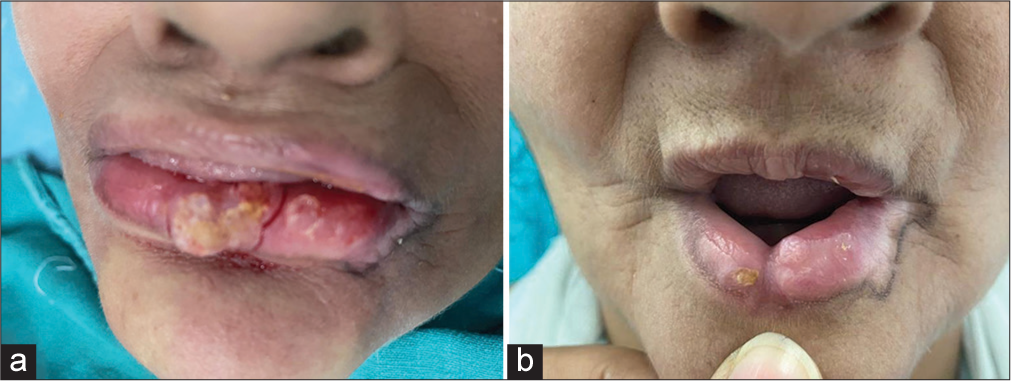
- (a) Before excision. (b) Post excision at 4 weeks.
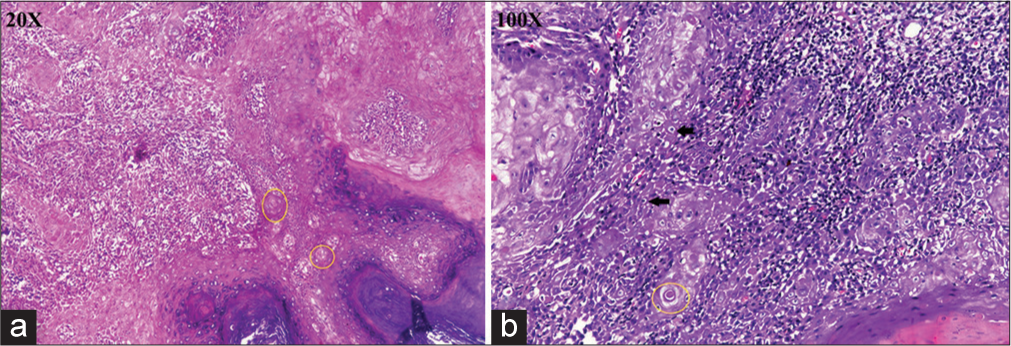
- (a) Histopathological examination at ×20 showing a hyperplastic and dysplastic epithelium with tumour cells. Tumour cells are moderately differentiated anaplastic squamous cells with hyperchromatic nuclei, inconspicuous nucleoli and moderate amount of cytoplasm. Keratin pearls are seen (yellow circles). (b) Histopathological examination at ×100 showing tumour cells (black arrows) and keratin pearls (yellow circles).
DLE patients are at higher risk of developing SCC and various risk factors have been associated including chronic immunosuppressive drugs, ultra-violet exposure, chronic inflammation, low melanin, human papilloma virus and chronic scarring. Skin pigmentation has a protective effect due to melanin but lower lip is more prone to develop changes due to direct photo exposure and deficiency of pigment.[1]
When the patient presents with clinical findings like long standing lesions, lesions at high risk sites (scalp, lips, face and forearm), lesions showing rapid evolution and morphology such as raised, hyperkeratotic, verrucous, ulcerative and erosive lesion with resistance to conventional treatment the lesion should be kept under surveillance. Histopathologic clues toward malignant transformation depicting verruca like or epitheliomatous hyperplasia like findings should also encourage the clinician to take a step back from mainstream management protocols and planned for wide local excision.
Similar cases where histopathology at initial instance reported hypertrophic or verrucous changes but on follow-up showed features of moderately or poorly differentiated SCC have been reported.[5] It was observed in our case that biopsies at interval of few months showed varied findings suggesting that if and whenever feasible excision must be planned for such lesions as incisional biopsy may miss areas undergoing malignant transformation.
To conclude, histopathological findings of SCC in excised DLE lesion teach that excision of such long-standing DLE lesions is more beneficial and accurate as both a diagnostic and therapeutic measure.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Discoid Lupus Erythematosus leading to Squamous Cell Carcinoma. Med J Armed Forces India. 2007;63:184-5.
- [CrossRef] [PubMed] [Google Scholar]
- Chronic Inflammation Promotes Skin Carcinogenesis in Cancer-Prone Discoid Lupus Erythematosus. J Invest Dermatol. 2019;139:62-70.
- [CrossRef] [PubMed] [Google Scholar]
- Disseminated Discoid Lupus Erythematosus Leading to Squamous Cell Carcinoma. Indian J Dermatol. 2012;57:158-61.
- [CrossRef] [PubMed] [Google Scholar]
- Surgical Excision of Trauma-induced Verrucous Lupus Erythematosus. J Dermatol Surg Oncol. 1988;14:1296-9.
- [CrossRef] [PubMed] [Google Scholar]
- Squamous Cell Carcinoma Developing in Two Chinese Patients with Chronic Discoid Lupus Erythematosus: The Need for Continued Surveillance. Clin Exp Dermatol. 2006;31:542-4.
- [CrossRef] [PubMed] [Google Scholar]




