

Translate this page into:
Erythema Annulare Centrifugum as Indicator of Internal Malignancy
*Corresponding author: Gopalsing Rameshsing Rajput, Department of Dermatology, Institute of Naval Medicine, INHS Asvini, Mumbai, Maharashtra, India. gopal.270985@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Rajput GR, Hemdani R, Kaur C, Kharayat V. Erythema Annulare Centrifugum as Indicator of Internal Malignancy. Indian J Postgrad Dermatol. 2025;3:77-8. doi: 10.25259/IJPGD_69_2024
A 46-year-old male presented with well-defined annulare plaque with central clearing over right dorsum of hand, nape of neck and buttocks since 3 months [Figure 1a-c]. The lesions were accompanied by itching. He was being treated as case of dermatophyte infection with topical and systemic antifungal without much relief. Dermoscopy of lesions revealed whitish trailing scale with advancing erythematous edge [Figure 1d]. Potassium hydroxide (KOH, 10%) mount was negative. The histopathology of lesion revealed mild spongiosis, parakeratosis and minimal perivascular and periappendegeal lymphocytic infiltrate in upper dermis [Figure 2a]. He was labelled as a case of erythema annulare centrifugum (EAC). He had history of weight loss in past 3 months accompanied by non-productive cough. High-resolution computed tomography chest revealed large mass in the right upper lobe [Figure 2b and c]. His lung positron emission tomography scan revealed uptake in the upper right lobe [Figure 2d]. He was diagnosed as case of small-cell lung carcinoma. This image depicts the possibility of EAC in patients with figurate erythema morphology which on age-appropriate malignancy screen can result in early diagnosis of internal malignancy. These images also depict the importance of dermoscopy in differentiating tinea infection from EAC in busy outpatient department days.

- Well-defined annular plaque with central clearing and trailing scale and advancing erythematous border over dorsum of (a) the right hand, (b) buttock and (c) nape of neck, (d) dermoscopy of lesion showing whitish scale with advancing erythematous border (DermLite dl3 gen, ×10 magnification, Made in USA).
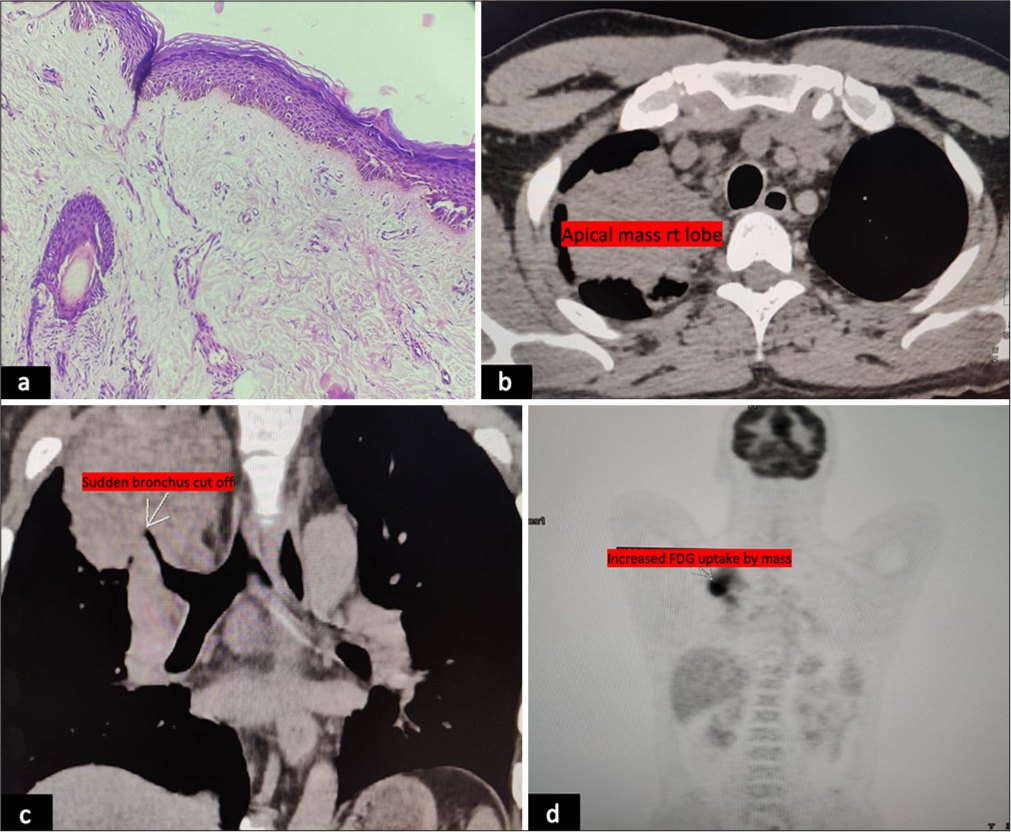
- Histopathological examination showing orthokeratosis, minimal (a) spongiosis along with minimal perivascular and periadnexal lymphocytic infiltrate (Haematoxylin and eosin, ×100), (b and c) high-resolution computed tomography showing mass in the right upper lobe of lung and (d) positron emission tomography scan showing avid uptake in the upper lobe of the right lung.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.




